Another publication, this time on the role of the ABI as a predictor for stroke recurrence. This is a meta analysis, which combines data from 11 studies allowing us to see that ABI was moderately associated with recurrent stroke (RR1.7) and vascular events (RR 2.2). Not that much, but it might be just enough to increase some of the risk prediction models available for stroke patients when ABI is incorperated.
This work, the product of the great work of some of the bright students that work at the CSB (JBH and COL), is a good start in our search for a good stroke recurrence risk prediction model. Thiswill be a major topic in our future research in the PROSCIS study which is led by TGL. I am looking forward to the results of that study, as better prediction models are needed in the clinic especially true as more precise data and diagnosis might lead to better subgroup specific risk prediction and treatment.
Another article got published today in the JAMA Int Med, this time the results from the first analyses of the RATIO follow-up data. For these data, we linked the RATIO study to the dutch national bureau of statistics (CBS), to obtain 20 years of follow-up on cardiovascular morbidity and mortality. We first submitted a full paper, but later we downsized to a research letter with only 600 words. This means that only the main message (i.e. cardiovascular recurrence is high, persistent over time and disease specific) is left.
It is a “Leiden publication”, where I worked together with AM and FP from Milano. Most of the credit of course goes to AM, who is the first author of this piece. The cool thing about this publication is that the team worked very hard on it for a long time (data linking and analyses where not an easy thing to do, as well as changing from 3000 words to 600 in just a week or so), and that in the end all the hard work paid off. But next to the hard work, it is also nice to see results being picked up by the media. The JAMA Int Med put out an international press release, whereas the LUMC is going to publish its own Dutch version. In the days before the ‘online first’ publication I already answered some emails from writers for medical news sites, some with up to 5.000K views per month. I do not know if you think that’s a lot, but for me it is. The websites that cover this story can be found here (dagensmedisin.se, healio.com, medicaldaily.com, medpagetoday.com, medonline.at, drugs.com / healthday.com / webmd.com / usnews.com / doctorslounge.com, medicalxpress.com, medicalnewstoday.com, eurekalert.org and perhaps more to come. Why not just take a look at the Altmetric of this article).
– edit 26.11.2015: a dutch press release from the LUMC can be found here) – edit: oops, medpagetoday.com has a published great report/interview, but used a wrong title…”Repeat MI and Stroke Risks Defined in ‘Younger’ Women on Oral Contraceptives”. not all women were on OC of course.
The article, with the full title “Recurrence and Mortality in Young Women With Myocardial Infarction or Ischemic Stroke: Long-term Follow-up of the Risk of Arterial Thrombosis in Relation to Oral Contraceptives (RATIO) Study“ can be found via JAMA Internal Medicine or via my personal Mendeley page.
So, it is just over a year since I started here in Berlin. In this year I had the opportunity to start some great projects. Some of these projects have already resulted in some handsome -upcoming- publications.
For those who wonder, the picture gives a somewhat inflated impression of the size of the team, as we decided to include all people who currently work with us. This includes two of our five students and 2 virchow scholars that are visiting from Amsterdam and Hamburg. I included them all in the picture, as I enjoy my work here in Berlin because of all team members. Now, let’s do some science!
This is one of the first projects that I was involved with from start to finish since my start in Berlin to be published, so I’m quite content with it. A cool landmark after a year in Berlin.
Together with TL and LN I supervised a student from the Netherlands (JH). This publication is the result of all the work JH did, together with the great medical knowledge from the rest of the team. About the research: Posterior reversible encephalopathy syndrome, or PRES, is a syndrome that can have stroke like symptoms, but in fact has got nothing to do with it. The syndrome was recognised as a separate entity only a couple of years ago, and this group of patients that we collected from the Charite is one of the largest collections in the world.
It is a syndrome characterised by edema (being either vasogenic or cytotoxic), suggesting there is something wrong with the fluid balance in the brain. A good way to learn more about the fluids in the brain is to take a look at the different things you can measure in the cerebrospinal fluid. The aim of this paper was therefore to see to what extend the edema, but also other patients characteristics, was associated with CSF parameters.
Our main conclusion is indeed the total amount of protein in the CSF is elevated in most PRES patients, and that severe edema grade was associated with more CSF. Remind yourself that this is basically a case series (with some follow up) but CSF is therefore measured during diagnosis and only in a selection of the patients. Selection bias is therefore likely to be affecting our results as well as the possibility of reverse causation. Next to that, research into “syndromes” is always complicated as they are a man-made concept. This problem we also encountered in the RATIO analyses about the antiphospholipid syndrome (Urbanus, Lancet Neurol 2009): a real syndrome diagnosis could not be given, as that requires two blood draws with 3 months time in between which is not possible in this case-control study. But still, there is a whole lot of stuff to learn about the syndromes in our clinical research projects.
I think this is also true for the PRES study: I think that our results show that it is justified to do a prospective and rigorous and standardised analyses of these patients with the dangerous syndrome. More knowledge on the causes and consequences is needed!
The paper can be cited as:
Neeb L, Hoekstra J, Endres M, Siegerink B, Siebert E, Liman TG. Spectrum of cerebral spinal fluid findings in patients with posterior reversible encephalopathy syndrome. J Neurol; 2015; (e-pub) and can be found on pubmed or on my mendeley profile
Together with several co-authors, with first author AN in the lead, we did a meta analyses on the role of Lp(a) as a risk factor of stroke. Bottomline, Lp(a) seems to be a risk factor for stroke, which was most prominently seen in the young.
The results are not the only reason why I am so enthusiastic by this article. It is also about the epidemiological problem that AN encountered and we ended up discussing over coffee. The problem: the different studies use different categorisations (tertiles, quartiles, quintiles). How to use these data and pool them in a way to get a valid and precise answer to the research question? In the end we ended up using the technique proposed used by DDanesh et al. JAMA. 1998;279(18):1477-1482 that uses the normal distribution and the distances in SD. A neat technique, even though it assumes a couple of things about the uniformity of the effect over the range of the exposure. An IPD would be better, as we would be free to investigate the dose relationship and we would be able to keep adjustment for confounding uniform, but hey… this is cool in itself!
I just got word that I am elected as fellow of the European Stroke Organisation. Well, elected sounds more cool then it really is… I applied myself by sending in an application letter, resume, some form to show my experience in stroke research and two letters of recommendation of two active fellows and that’s that. So what does this mean? Basically, the fellows of the ESO are those who want to put some of their time to good use in name of the ESO, such as being active in one fo the committees. I chose to get active in teaching epidemiology (teaching courses during the ESOC conferences, or in the winter/summer schools, perhaps in the to be founded ESO scientific journal), but how is as of this moment not completely clear yet. Nonetheless, I am glad that I can work with and through this organisation to improve the epidemiological knowledge in the field of stroke.
Ischaemic stroke + myocardial infarction = arterial thrombosis. Are these two diseases just two sides of the side coin? Well, most if the research I did in the last couple of years tell a different story: most times,hypercoagulability has a stronger impact on the risk of ischaemic stroke at least when compared to myocardial infarction. And when in some cases this was not the case, at least it as clear that the impact was differential. But these papers I published were all single data dots, so we needed to provide an overview of all these data points to get the whole picture. And we did so by publishing two papers, one in the JTH and one in PLOS ONE.
The first paper is a general discussion of the results from the RATIO study, basically an adaptation from my discussion chapter of my thesis (yes it took some time to get to the point of publication, but that’s a whole different story), with a more in-depth discussion to what extent we can draw conclusions from these data. We tried to fill in the caveats (limited number of markers, only young women, only case-control, basically single study) of the first study with our second publication. Here we did the same trick, but in a systematic review.This way, our results have more external validity, while we ensured the internal validity by only including studies that studied both diseases and thus ruling out large biases due to differences in study design. I love these two publications!
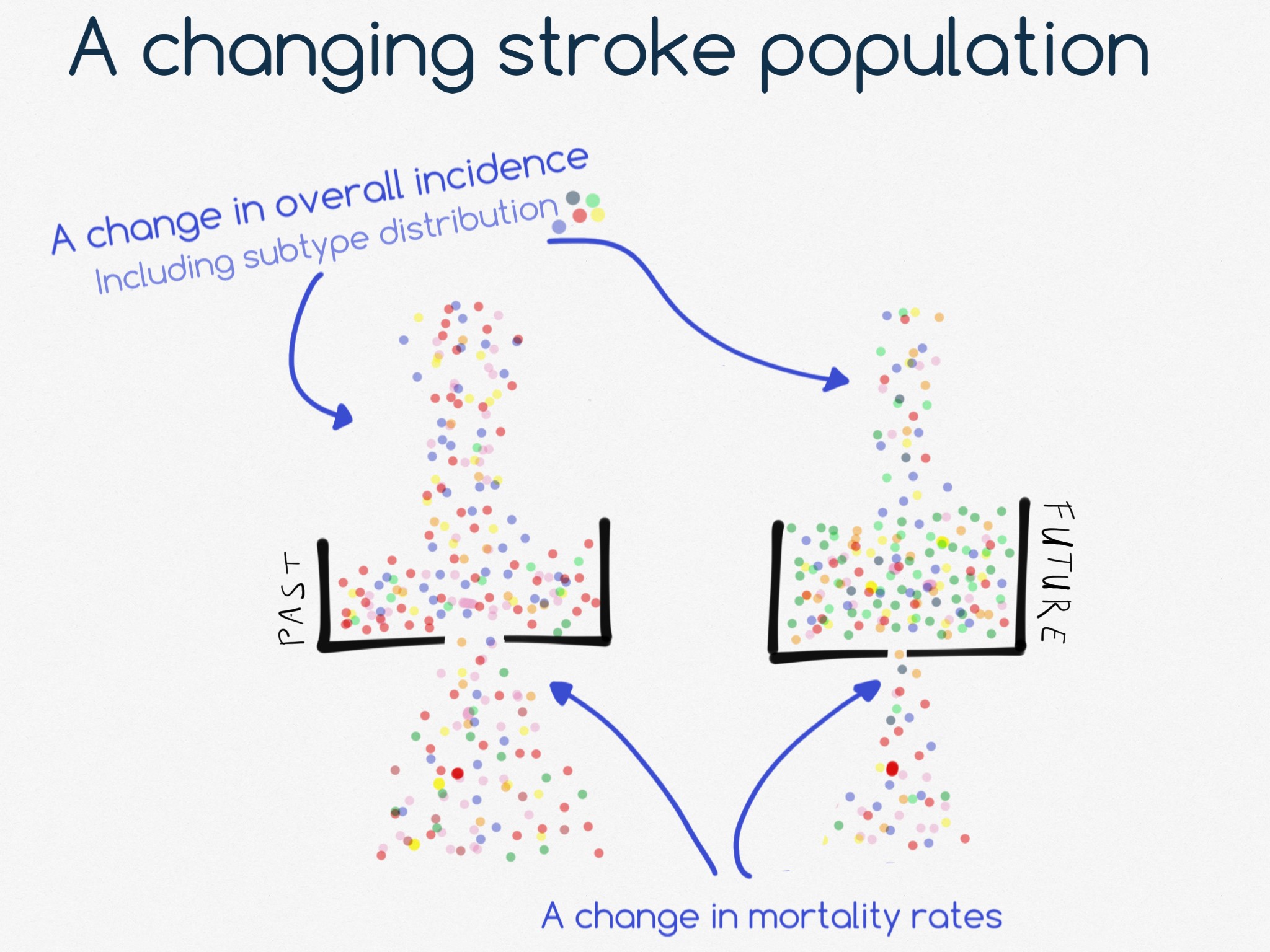
Lower changing incidences of disease over time do not necessarily mean that the number of patients in care also goes down, as the prevalence of the disease is a function of incidence and mortality. “Death Cures”. Combine this notion with the fact that both the incidence and mortality rates of the different stroke subtypes change different over time, and you will see that the group of patients that suffer from stroke will be quite different from the current one.
I made this picture to accompany a small text on declining stroke incidences which I have written for the newsletter of the Kompetenznetz Schlaganfall. which can be found in this pdf.








{kind=link}