
The ISTH is a bi-annual conference on thrombosis and haemostasis, and this year it convenes in Toronto. We started yesterday with the SSCs which were interesting, but I am mainly looking forward to some of the sessions in the normal program. As is in line with the announcement 2 years ago, the organising committee strived to include more fields of medicine into the program, one being stroke. There even a couple of stroke themed sessions. Good!
Another topic that has my interest is the link between inflammation and coagulation. This link, perhaps through the intrinsic coagulation proteins, or perhaps through extracellular nucleic acids is quite interesting, as it might provide insight into the link between these two major biological systems that interact in the acute phase of stroke. Next to the SSC meeting this morning and yesterday, there are some plenaries and symposia on this topic; Tuesday seems to be the day for this!
I contributed to three papers that will be presented here, being:
ADAMTS13 AND THE RISK OF MYOCARDIAL INFARCTION: AN INDIVIDUAL PATIENT DATA META-ANALYSIS Alberto Maino*, Bob Siegerink, Luca Lotta, James Crawley, Saskia le Cessie, Frank Leebeek, David Lane, Gordon Lowe, Flora Peyvandi, Frits Rosendaal (Italy)
RECURRENCE AND MORTALITY IN YOUNG WOMEN WITH MYOCARDIAL INFARCTION OR ISCHEMIC STROKE: 19-YEAR FOLLOW-UP OF THE RISK OF ARTERIAL THROMBOSIS IN RELATION TO ORAL CONTRACEPTIVES (RATIO) STUDY. Alberto Maino*, Bob Siegerink, Ale Algra, Flora Peyvandi, Frits Rosendaal (Italy)
STATIN USE AND RISK OF RECURRENT VENOUS THROMBOSIS: RESULTS FROM THE MEGA FOLLOW-UP STUDY Willem Lijfering*, Sigrid Braekkan, Camilla Caram-Deeelder, Bob Siegerink, Astrid van Hylckama Vlieg, Saskia le Cessie, Frits Rosendaal, Suzanne Cannegieter (The Netherlands)
As a last thing: It was a last decision to join this conference, but I am happy I did. the scientific program helps, but more importantly, the Barenaked Ladies are going to perform at the conference party!
Ps one thing that is also quite interesting, but i only saw one oral communication on this, is the authophagy of clots… how cool is that! Keep the blood flowing in the microvasculature!







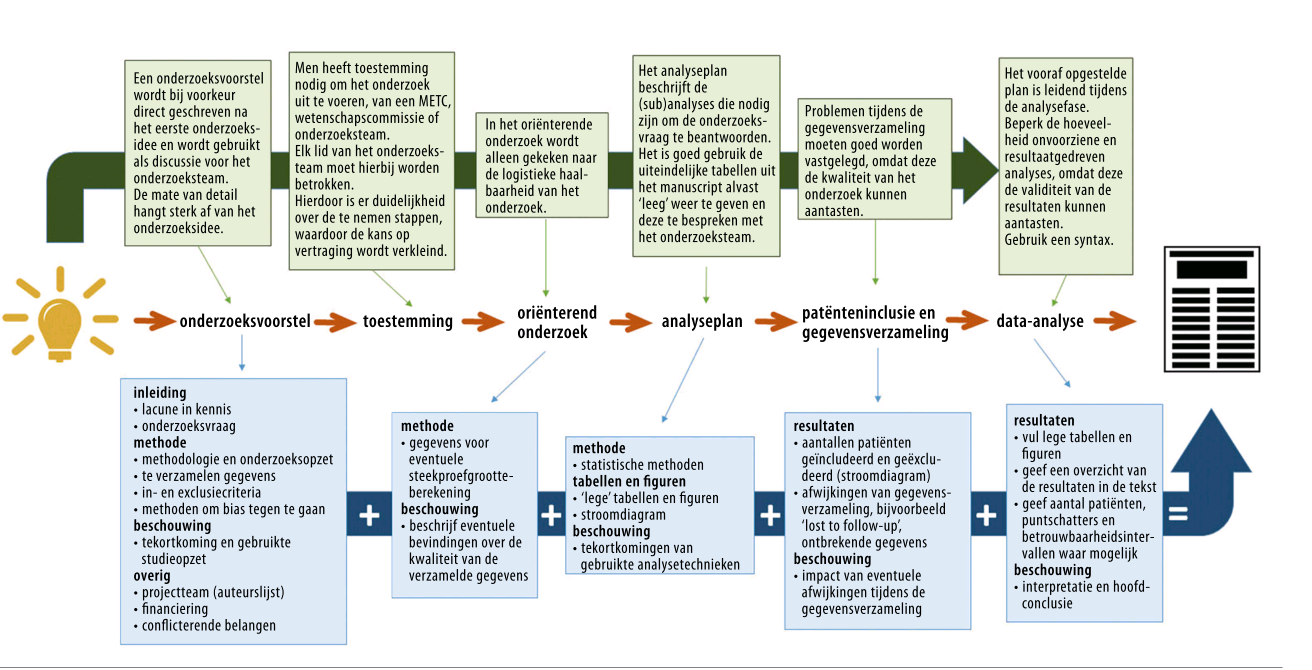






 After our first pilot of our workshop ‘
After our first pilot of our workshop ‘





